Article Text

Abstract
Background In patients who have been mechanically ventilated, inspiratory muscles remain weak and fatigable following ventilatory weaning, which may contribute to dyspnoea and limited functional recovery. Inspiratory muscle training may improve inspiratory muscle strength and endurance following weaning, potentially improving dyspnoea and quality of life in this patient group.
Methods We conducted a randomised trial with assessor-blinding and intention-to-treat analysis. Following 48 hours of successful weaning, 70 participants (mechanically ventilated ≥7 days) were randomised to receive inspiratory muscle training once daily 5 days/week for 2 weeks in addition to usual care, or usual care (control). Primary endpoints were inspiratory muscle strength and fatigue resistance index (FRI) 2 weeks following enrolment. Secondary endpoints included dyspnoea, physical function and quality of life, post-intensive care length of stay and in-hospital mortality.
Results 34 participants were randomly allocated to the training group and 36 to control. The training group demonstrated greater improvements in inspiratory strength (training: 17%, control: 6%, mean difference: 11%, p=0.02). There were no statistically significant differences in FRI (0.03 vs 0.02, p=0.81), physical function (0.25 vs 0.25, p=0.97) or dyspnoea (−0.5 vs 0.2, p=0.22). Improvement in quality of life was greater in the training group (14% vs 2%, mean difference 12%, p=0.03). In-hospital mortality was higher in the training group (4 vs 0, 12% vs 0%, p=0.051).
Conclusions Inspiratory muscle training following successful weaning increases inspiratory muscle strength and quality of life, but we cannot confidently rule out an associated increased risk of in-hospital mortality.
Trial registration number ACTRN12610001089022, results.
- Respiratory Muscles
- Exercise
- Respiratory Measurement
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Key messages
What is the key question?
Does inspiratory muscle training enhance recovery for patients who have been invasively ventilated for 7 days or longer?
What is the bottom line?
Two weeks of daily supervised inspiratory muscle training significantly improves inspiratory muscle strength and health-related quality of life in patients recently weaned from invasive ventilation.
Why read on?
Understand how this specific regime of inspiratory muscle training may be a useful adjunct to the medical management of patients in the postweaning period.
Introduction
Invasive mechanical ventilation causes respiratory muscle weakness in intensive care unit (ICU) patients.1 After 18–69 hours of controlled mechanical ventilation, diaphragm proteolysis and atrophy occur1 and respiratory muscle weakness has been observed both while patients are mechanically ventilated2 and following successful extubation.3 ,4 Persistent respiratory muscle weakness may contribute to the residual dyspnoea,4 impaired physical function4 ,5 and poor quality of life6 observed in ICU survivors.
Inspiratory muscle training (IMT) is a relatively novel training strategy to improve inspiratory muscle strength in ICU patients. Threshold-based IMT is performed using a handheld device, which provides carefully titrated constant resistance on inspiration only. A preset threshold level of pressure is required to open a one-way valve and allow inspiratory flow, which is important in ensuring accurate titration of resistance as some other IMT devices are flow-dependent, which means that the resistance varies with patient effort. Using a threshold IMT device the level of inspiratory pressure required to open the valve is increased over time to provide an ongoing training load as the patient's inspiratory muscles become stronger. IMT improves respiratory muscle strength in patients undergoing invasive mechanical ventilation7–11 and a recent systematic review suggested that IMT performed prior to extubation enhances weaning success, although it does not appear to reduce rates of reintubation or likelihood of survival.12
However, participation in threshold-based IMT while mechanically ventilated requires patients to be alert and cooperative with training.13 For many reasons, ICU patients may not be suitable candidates for IMT while ventilator-dependent (eg, due to sedation or delirium) and may only have sufficient cognitive capacity to participate in training once weaned from mechanical ventilation. Although case studies have shown improvements in inspiratory muscle strength with IMT,14 there have been no randomised trials of IMT in ICU patients in the postextubation period.
As residual inspiratory muscle impairment has been demonstrated in intensive care survivors ventilated for 7 days or longer,3 ,4 we conducted a randomised trial to establish the effects of postextubation IMT in a heterogeneous sample of ICU patients who had been invasively ventilated for at least 7 days. Primary endpoints included inspiratory muscle strength and endurance following 2 weeks of training. This 2 week time frame was selected pragmatically, as pilot data indicated that most intensive care survivors remained inpatients during this 2 week period and would receive supervised physiotherapy. To date, no studies of IMT in ICU patients have included patient-centred outcomes or rates of readmission to ICU. Therefore, secondary endpoints included health-related quality of life, dyspnoea and functional levels after 2 weeks of training. Post-intensive care length of stay, rate of intensive care readmission and in-hospital mortality were also explored. We hypothesised that in the IMT group, improvements in inspiratory muscle strength and fatigue resistance would lead to reduced dyspnoea, improved quality of life and physical function, and lower rates of intensive care readmission and in-hospital mortality compared with the control group.15
Methods
Design
We conducted a single-centre randomised trial with concealed allocation (computer-generated random-number sequence, managed by off-site administrative staff and obtained via telephone by the chief investigator following enrolment), assessor-blinding and intention-to-treat (ITT) analysis.15 The study was approved by the Australian Capital Territory Health Human Research Ethics Committee and the University of Queensland Medical Research Ethics Committee, and the published study protocol15 (trial registration ACTRN12610001089022) complied with the CONSORT guidelines for clinical trials.16
Participants, therapists, centre
All patients invasively mechanically ventilated for 7 days or longer were screened for eligibility. Patients were deemed eligible if they had been successfully weaned from mechanical ventilation (>48 hours), and within the 7 days following successful weaning they met the inclusion criteria (aged ≥16 years, able to provide informed consent, and alert and able to participate in training with a Riker17 score of 4). Patients were excluded if they had participated in IMT while mechanically ventilated, declined to participate, were pregnant, were not alert or able to participate with training, were experiencing significant pain or distress that interfered with breathing capacity and were deemed medically unstable or for palliation (ie, death likely in the next few weeks). Based on a priori power calculations, a total of 70 participants were required to detect a 0.10 change in the primary outcome measures with a power of 0.80 (inflating group size by 15% to allow for known mortality of 12.8%15). Although the minimal clinically important difference in maximum inspiratory pressure (MIP) scores has not been established in this patient group, the 0.10 change level was selected based on previous studies of inspiratory muscle strength and fatigue resistance in intensive care survivors3 ,14 to allow comparisons to be drawn between studies. All participants provided informed written consent to participate in the study.
Training was supervised by registered physiotherapists specifically trained in delivering IMT as described in our previously published protocols.13 ,15 Therapists could not be blinded to group allocation. The study was conducted in an Australian tertiary hospital (Canberra Hospital) where usual intensive care practice includes minimal sedation and early proactive mobilisation.18 A second site was also included (Calvary Hospital); however, no patients were recruited from this site due to failure to meet eligibility requirements.
Intervention
Participants were randomised to receive either usual care (control group) or IMT in addition to usual care (IMT group) for 2 weeks following enrolment. Usual care physiotherapy included an individually tailored and supervised programme of interventions, which included any of the following: assisted mobilisation, secretion clearance treatments including positive expiratory pressure techniques, deep breathing exercises without a resistance device and upper and lower limb exercises.
IMT was performed using the threshold IMT inspiratory muscle trainer (threshold IMT device HS730, Respironics, New Jersey, USA). This device was used with the mouthpiece, or a flexible connector if required to attach to a tracheostomy (figure 1). Where a tracheostomy remained in situ, IMT was always performed with the cuff inflated to ensure accurate loading. The physiotherapist prescribed an intensity of 50% of MIP for the first training set, but then quickly increased this to the highest tolerable intensity that allowed the participant to just complete the sixth breath in a set of six breaths, with five sets of six breaths completed each session. Patients were allowed to rest between sets until they felt ready to commence the next set, which was typically less than 1 min of resting. The intensity was increased daily by the physiotherapist across the training period to provide an adequate training stimulus. This was achieved by manually increasing the threshold resistance by 1–2 cm H2O until the participant could only just open the poppet valve on the sixth breath in each set. Training commenced on the day of enrolment and continued once daily (weekdays only) for 2 weeks. A sham device was not used for comparison as previous studies of IMT have found that the sham device may provide a training effect in participants with very low baseline strength.19

Inspiratory muscle training via a tracheostomy. Note the flexible tubing connecting the inspiratory muscle trainer to the closed suction device.
Measures
Primary endpoints
Measures of inspiratory muscle performance were recorded on enrolment and at the end of the intervention period 2 weeks later by six specifically trained research nurses blinded to group allocation. Inspiratory muscle strength was assessed as MIP, measured as previously described15 using a portable MicroRPM Respiratory Pressure meter (CareFusion, San Diego, USA) in accordance with the protocol described by the American Thoracic Society and European Respiratory Society.20 This device has been shown to have excellent reliability in measuring MIP in non-ventilated participants (intraclass correlation coefficient 0.83–0.90).21 Raw MIP scores were normalised using the method described by Evans and Whitelaw22 and have been presented as percentage of predicted values to account for known variation of MIP with age and gender. Inspiratory muscle fatigue was measured using the fatigue resistance index (FRI) technique described by Chang and colleagues,3 based on the maximum incremental threshold loading test described in the American Thoracic Society/European Respiratory Society guidelines.23The prespecified endpoint was the between-group difference in change in outcome measures (ie, the change from enrolment to 2 week follow-up values).
Secondary endpoints
Measures of quality of life, dyspnoea and physical function were completed on enrolment and 2 weeks later. Quality of life was measured using the SF-36v2 tool (acute 1 week time frame) (under license Quality Metric USA) and the EQ-5D-3L tool (under license EuroQol International). These tools were administered by research nurses blinded to group allocation. The SF-36 tool has demonstrated reliability, responsiveness, construct and criterion validity and is responsive to clinical improvement in an intensive care population.24 The EQ-5D-3L tool has also been used in intensive care patient follow-up25 and is likely to give a more general measure of health-related quality of life than the SF-36.
Dyspnoea was measured using a Modified Borg Dyspnoea scale, where dyspnoea is a patient-reported categorical score out of 10, which has acceptable reliability and validity in patients undergoing mechanical ventilation.26 Dyspnoea was recorded both at rest (sitting comfortably in the chair or bed) and during exercise (the peak exercise activity experienced in the previous 24 hours) by research nurses blinded to group allocation.
Functional level including mental status, bed mobility, transfers and mobility was assessed using the acute care index of function (ACIF),27 which has excellent inter-rater reliability in ICU patients.28 Scores on enrolment were completed by physiotherapists blinded to group allocation; however, follow-up ACIF scores were recorded by the treating physiotherapist who was not blinded to group allocation.
Other secondary endpoints included rate of ICU readmission, requirement for reintubation, post-ICU hospital length of stay and in-hospital mortality. These data were extracted from hospital databases by research nurses blinded to group allocation. Post hoc analysis of participants who died during the hospital admission included retrospective calculation of the risk of death based on acute physiology and chronic health evaluation (APACHE II) scores.
Data analysis
The ITT population was defined as all 70 randomised participants. The per-protocol population was defined as all participants with both enrolment and 2 week follow-up data. All analyses were repeated in both the ITT and per-protocol populations. Paired t-tests were used to compare within-group differences. Mixed linear models were used to assess the between-group difference of the changes between enrolment and follow-up measures, including age and APACHEII scores as covariates. Diagnostic plots (predicted means vs Pearson’s residuals) were generated to assess model assumptions. Mortality data were analysed using χ2 and Fisher's exact test. Statistical significance was set as p<0.05. All analyses were done using SPSS V.21.
Results
Flow of participants through the study
The flow of participants is presented in figure 2. Between February 2011 and August 2015, 70 participants were recruited to participate in the study with 34 allocated to the IMT group and 36 to the control group. Participant characteristics are presented in table 1 and are similar between IMT and control groups, except for a higher percentage of male participants in the IMT group (71% vs 58%).
Characteristics of participants

Flow of participants through study. ACIF, acute care index of function; CVA, cerebrovascular accident; FRI, fatigue resistance index; ICU, intensive care unit; IMT, inspiratory muscle training; MIP, maximum inspiratory pressure; QOL, quality of life; RPE, rate of perceived exertion; TBI, traumatic brain injury.
The most frequent reason for exclusion from the study was poor neurological status with resultant inability to provide consent. Six participants were lost to follow-up in each group, most commonly due to transfer to another hospital within the study period. Two participants died within the intervention period, both in the IMT group. Two participants died after the intervention but prior to hospital discharge, both in the IMT group. Thus, the total mortality in the treatment group was 12%, compared with 0% in the control group. Where patients were lost to follow-up regarding the primary outcome measures, other postintervention secondary measures were still obtained through hospital databases (table 3).
Compliance with trial protocol
In the IMT group, across the 34 participants, 85% of all intended IMT treatments (potential 10 treatments for each patient) were completed. Twenty-three participants (67%) completed more than 90% of the prescribed IMT sessions, while two (6%) participants completed 20% or less of the prescribed IMT sessions. The most frequent reason for lack of completion was participant refusal due to generalised fatigue. IMT was generally well tolerated and no adverse effects were reported during or immediately after training in any participant. No participants in the control group inadvertently received IMT. Two participants (both in the control group) were discharged home prior to completion of the 2 week intervention period; however, they attended the outpatient department for completion of outcome measures.
Effect of intervention
The ITT and per-protocol analyses yielded entirely congruent results; therefore, only the ITT analysis is presented. Changes in outcome measures within and between groups are summarised in online supplementary table E1 and table 2. MIP improved in both groups, with a statistically significant greater increase in the IMT group than the control group (17% in IMT group vs 6% in control, p=0.024) (figure 3A). No statistically significant change in FRI was observed for either group at the end of the study period (0.03 vs 0.02, p=0.81) (figure 3B).
Differences within and between groups for each outcome measure at 2 weeks

Inspiratory muscle changes in both groups: (A) Changes in maximum inspiratory pressure scores before and after intervention. (B) Changes in fatigue resistance index before and after intervention. The box is drawn from the 25th percentile to the75th percentile, and the whiskers are drawn at 1.5 times IQR, with outliers represented with dots. IMT, inspiratory muscle training; MIP, maximum inspiratory pressure
Supplementary table
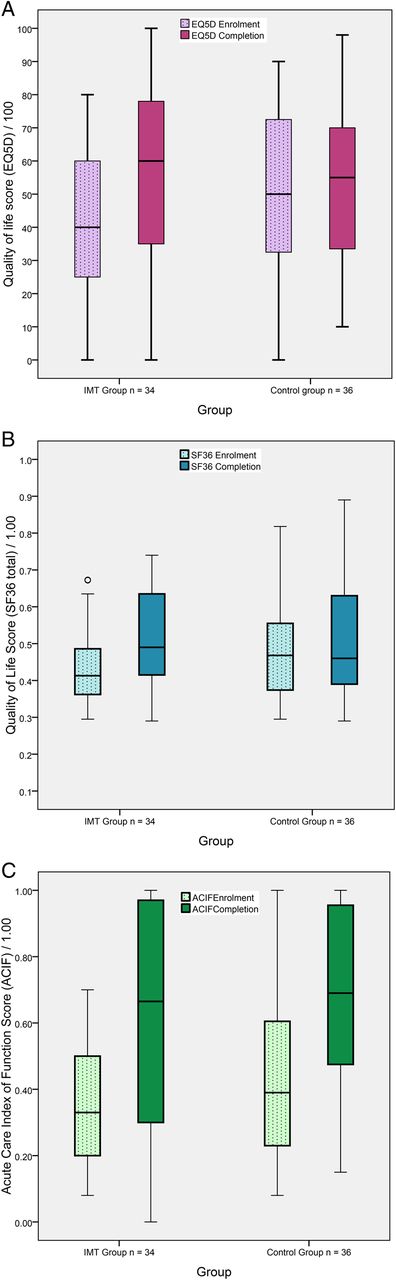
Both quality-of-life measures demonstrated statistically significant improvements from baseline in the IMT group only (mean difference=14, p=0.001 for EQ5D; mean difference=0.08, p=0.001 for SF-36) (figure 4A, B). Between groups, the difference in EQ5D scores was higher in the IMT group (14 vs 2, p=0.034). There was no statistically significant difference in SF-36 scores, although the point estimates suggested a potential benefit (mean difference=0.05, 95% CI=−0.01 to 0.10).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Quality of life and functional measures in both groups: (A) Changes in EQ5D scores before and after intervention. (B) Changes in SF36 scores before and after intervention. (C) Changes in acute care index of function before and after intervention. The box is drawn from the 25th percentile to the75th percentile, and the whiskers are drawn at 1.5 times IQR, with outliers represented with dots. FRI, fatigue resistance index; IMT, inspiratory muscle training
Both groups demonstrated significant improvements in functional outcomes, as measured by the ACIF (figure 4C); however, these improvements did not differ between groups (0.25 vs 0.25, p=0.974). Changes in dyspnoea scores both at rest and during exercise were not statistically significant either within or between groups across the intervention period.
There were no significant differences between groups for post-ICU length of stay, reintubation rate or ICU readmission (table 3). However, in-hospital mortality was higher in the IMT group (p=0.051) with four deaths, two during the 2 week intervention period and two following the intervention period (see online supplementary table E2 for details regarding causes of death).
Comparisons between groups for postintervention outcome measures
Discussion
We have shown for the first time that in the postextubation period, participants who complete 2 weeks of IMT have greater improvement in respiratory muscle strength than those who do not train. This is congruent with previous studies of IMT in mechanically ventilated patients8 ,10 ,11 and with the rapid strength gains within 2 weeks of commencing IMT previously described in healthy cyclists (eg, increased MIP scores by 8.4%29). It is possible that some of the apparent strength gains could be attributable to a learning effect, given the similarity between the IMT technique and the MIP testing manoeuvre. However, in ICU patients rapid atrophy has been observed in both skeletal30 and respiratory muscles1 within the first few days of admission. With an adequate training stimulus, some of these changes could be reversible within a relatively short time frame, although it appears that some individuals respond to training more than others (see online supplementary figure E1). Regardless of the underlying mechanism of improvement, the apparent strength gains in this cohort translated into benefits in quality of life, which is arguably a more important patient-centred outcome than inspiratory muscle strength.
Our inability to demonstrate an improvement in inspiratory muscle endurance in the IMT group is somewhat surprising, as IMT has been shown to increase proliferation of both type 1 and type 2 inspiratory muscle fibres31 and endurance benefits of IMT have been reported after 8 weeks of training in patients with COPD,32 after 11 weeks of training in athletes33 and after 4 weeks of training in recreationally active people.34 While it is possible that the specific training regime employed in our study translates into strength benefits alone, it is more likely that the duration of training was insufficient to affect a measurable improvement in endurance, or that the FRI is insufficiently sensitive to detect subtle changes in endurance over such a short time frame. A more sustained constant loading test may have better elucidated changes in inspiratory muscle endurance; however, our experience with these participants resonated with that of Chang and colleagues3 who found a limited tolerance for even the basic 2 min FRI test. Thus, measuring inspiratory muscle endurance in this patient group remains a challenge.
The statistically significant improvements in quality of life in the IMT group, as measured with the EQ5D tool (figure 4A), warrant further exploration. The magnitude of change in EQ5D scores (14 in the IMT group compared with two in the control) is likely to be clinically important in this group, which struggles with poor quality of life following weaning. While the IMT group commenced from a lower baseline EQ5D score (41 in the IMT group compared with 51 in the control) (see online supplementary table E1) we believe that it is unlikely that there was a ceiling effect in this cohort, as scores at 2 weeks remained well below maximal values (ie, mean 54% across both groups). We would expect quality of life to continue a slow trajectory of improvement beyond the ICU stay35 but it is possible that IMT provides an advantage early in this trajectory.
Although the IMT group expressed improved quality of life using the EQ5D tool, the effect was less marked when assessed by the SF36. This may reflect difficulty in completing all components of the longer SF36 questionnaire. One of the challenges in ICU outcomes research is the effect of residual cognitive impairment5 and fatigue on a participant's ability to complete lengthy quality-of-life assessment tools. The reasons for improved quality of life in the absence of a demonstrated effect on respiratory endurance, dyspnoea or functional level remain unclear.
Improvements in inspiratory muscle strength did not have a clinically or statistically significant impact on the other patient-centred outcomes in this study. While physical function improved similarly in both groups, it is likely that other aspects of treatment (eg, whole body exercise and gait retraining) had a stronger influence on recovery of physical function than IMT. The fact that both groups improved in terms of physical function may reflect the high standard of usual care in this unit, which includes early rehabilitation and mobilisation. Thus, the findings of this study may only be generalisable to acute settings where early mobilisation and rehabilitation are the norm. Furthermore, the failure of IMT to significantly affect reintubation rates or length of stay may be attributable to the small sample size, as the effect size of IMT may be very small in relation to the many other variables that impact on these clinically significant outcomes. Future studies of IMT in the postweaning period should be adequately powered to further clarify these relationships.
The difference in in-hospital mortality between groups was unexpected, although the mortality in the IMT group (12%) was close to that anticipated in the trial design (12.8%). To our knowledge, no increase in mortality has been reported with IMT in any population to date, including ventilated ICU patients, or patients with COPD or heart failure. As summarised in online supplementary table E2, none of the deaths appeared to be related directly to IMT or respiratory complications. Given the small number of study participants and heterogeneity of diagnoses, further study of the impact of IMT on in-hospital mortality is indicated before robust conclusions about mortality can be drawn.
Limitations of this study include a loss to follow-up of 17%, which should have been partly offset by the planned sample size augmentation of 15% to account for anticipated mortality. A lack of follow-up of primary outcomes beyond 2 weeks is another limitation. Moreover, some patients may benefit from ongoing IMT beyond a 2 week training period, particularly as most did not return to 100% of predicted MIP values during this study. In patients with COPD, IMT has longer-term benefits including lower rates of hospitalisation over a 12 month period.36 It is possible therefore that IMT in the postextubation period has ongoing effects, which should be assessed further.
With regard to the training device, a ceiling effect was problematic in two participants whose MIP exceeded 82 at baseline. As the maximum resistance setting on the device is 41 cm H2O, it was impossible to provide training at greater than 50% of MIP in these two participants. While all other participants commenced at 50% MIP intensity during the training period, 16 participants (47%) achieved the 41 cm H2O maximal setting on the device at some point during the 2 week period, limiting further incremental training. Thus, our study may have underestimated the potential impact of IMT. In future studies of IMT we recommend using a device with the capacity to provide higher training intensities, such as an electronic device.37 Furthermore, future studies may target those with identifiable strength deficits, as these may constitute a subgroup, which is most likely to benefit from training, while those with high baseline values have probably diluted the potential benefits of training in our cohort.
This study is the first to demonstrate the value of IMT for patients in the postextubation period. IMT can be considered an effective strategy to reverse some of the residual inspiratory muscle weakness, which is common following prolonged mechanical ventilation, and may enhance quality of life in these patients with just 2 weeks of training. Future studies of ICU patients in the postextubation period should further explore the impact of IMT on quality of life, as well as the longer term effects of IMT in this group, including effects on mortality.
Acknowledgments
The authors gratefully acknowledge the support of the physiotherapists of the Acute Support Physiotherapy Department at Canberra Hospital who provided the intervention, and the Canberra Hospital ICU research nurses (led by Ms Helen Rodgers).
References
Footnotes
Twitter Follow Bernie Bissett at @BernieBissett
Contributors BMB had full access to all of the data in the study and takes responsibility for the integrity of the data and the accuracy of the analysis. IAL substantially contributed to the study design, data analysis and interpretation, and the writing of the manuscript. RB and JP contributed substantially to the study design, data interpretation and the writing of the manuscript; TN substantially to the data analysis and the writing of the manuscript.
Funding We gratefully acknowledge the Canberra Hospital Private Practice Fund (2010) and the Canberra Hospital Auxiliary Research Fund for supporting this study. We also gratefully acknowledge the support of the University of Canberra Health Research Institute.
Competing interests None declared.
Ethics approval This study was approved by the Australian Capital Territory Health Human Research Ethics Committee (ETH.10.10.370) and the University of Queensland Medical Research Ethics Committee (2010001488).
Provenance and peer review Not commissioned; externally peer reviewed.